


|
1 |
The number of over-16s on a Child Protection Plans tripled between 2006 and 2009 (Brooks and Brocklehurst, 2010).The overall number of CPPs more than doubled (51%) between 2007-08 and 2011-12, including an eight per cent increase in 2011-12 alone (Brooks et al, 2012). There was a further 1.1% increase in 2012-13, all of which represents a huge increase in service demand over this six-year period (Children in Need Statistics, Department for Education). |
|
2 |
The 2010 Safeguarding Pressures report highlighted a 132 per cent increase in the number of looked after young people aged 16 and over (Brooks and Brocklehurst, 2010). |
|
3 |
Statistical evidence examining age-related patterns in referrals and initial assessments show that referrals of older children and young people ‘appear to be significantly less likely to go down a child protection route’ (Rees et al 2010). |
|
4 |
23% of SCRs between 2003 and 2009 involved a young person aged 11 to 17 years at the time of the incident, with girls over-represented in these older age groups (Source: Brandon et al 2010) |
|
5 |
The 2012 biennial analysis of SCRs from 2009-11 found a similar overall percentage related to 11-17-year-olds; however, there were more boys than girls in the 11-15 age group and theresearchers report no clear pattern of gender distribution for this age group across SCRs between 2005 and 2011 (Source:Brandon et al 2012) |
|
6 |
21% (n=55) of all SCR incidents 2007-09 occurred outside the family in a community context (defined as ‘involving non-household/family members and gang/street-related violence’, with suicides of young people outside the family setting also included in this category (source: Brandon et al 2010).Girls (58%) were slightly over-represented. Of the 55 SCR incidents in a community setting, 35 involved young people aged 11 to 17. |
|
7 |
Key themes linked to the experiences of this age group included: street-level/gang-related violence; risky adolescent behaviour (including suicide and self-harm); the young person as perpetrator of the serious incident; incidents occurring in supervised settings (eg school, hospital or residential care); and sexual abuse by a perpetrator from outside the family. |
Why do teenagers seem so much more impulsive, so much less self-aware than adults?
In this TED Video, Cognitive neuroscientist Sarah-Jayne Blakemore compares the prefrontal cortex in adolescents to that of adults, to show us how typically "teenage" behavior is caused by the growing and developing brain.
In Summary, the emerging neurological evidence is improving our understanding of the best opportunities for intervention. Working with developmental factors enables us to increase the chances of success of a particular approach e.g adolescents’ limited ability to favour delayed rewards over immediate gains should be taken into account when considering the design of services and approaches to motivating young people to change. Focused and brief early intervention programmes to improve self-control are promising and can help reduce delinquency and problem behaviours for children up to age 12 (Research in Practice).
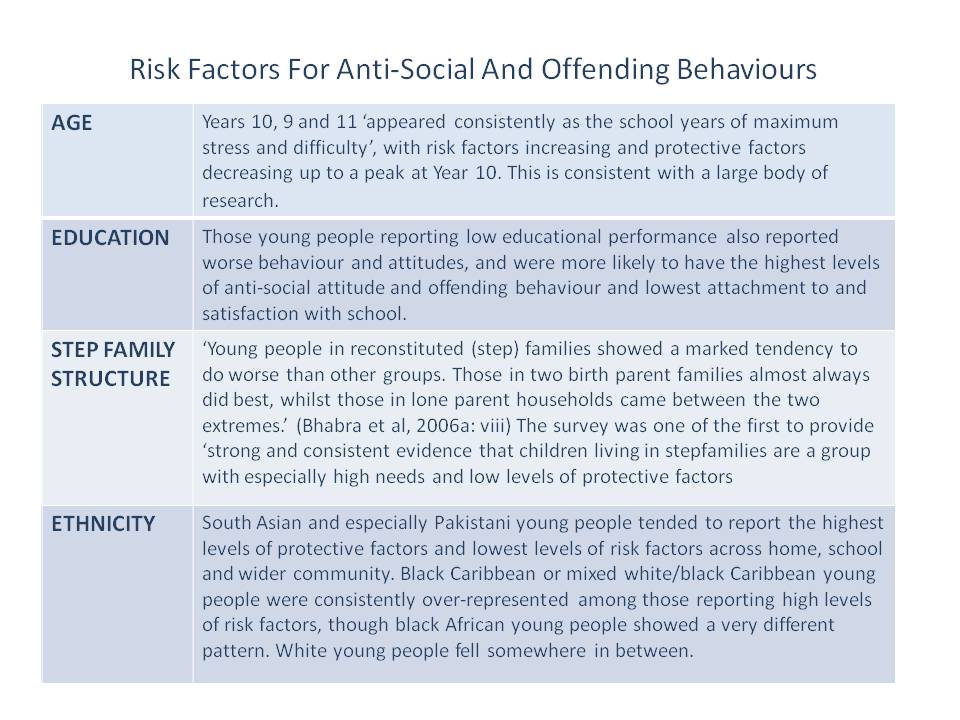
Risk Factors for Anti-Social and Offending Behaviours
On Track: a multi-component initiative aimed at children and families that might be at risk of offending. The national evaluation of On Track (Bhabra et al, 2006a) included a large-scale survey of 12,700 pupils in school in 24 areas of high crime and deprivation. Around one in ten of the young people surveyed were at risk of anti-social behaviour and other poor outcomes (reporting five or more of the following risk factors: parental tolerance of antisocial behaviour, siblings with anti-social behaviour, peers with anti-social behaviour, their own attitudes to anti-social behaviour, school exclusion, truancy, offending, challenging attitudes). The On Track survey findings give a sense of young people’s own perceptions of the risks they face. Download the full On Track Evaluation Report HERE.
Adolescents at Risk of Harm
Adolescents as people, and adolecence as a a stage of development, are often subject to a range of assumptions and myths. How often has the term "typical adolescent" been used as a general description of a young person: their apprearance, their behaviour and their interests? More often such a term has negative connotations and is an attempt to explain a difficulty or challenge that the young person presents to parents, carers, teachers, and maybe even social workers!
In working with young people there are many contexts in which risk is an important consideration. A combination of factors in a young person’s system (their family, peer group, school or community) can make it more likely they will be exposed to risks or engage in risk-taking activities. Thus ‘risky’ behaviours may be precipitated by risk factors such as running away; possiblye the taking of one risk to escape another (such as maltreatment at home).
Risky and impulsive behaviour are a normal part of the teenage experience. With support, most young people navigate these challenges and emerge as healthily functioning adults. However, the interaction of individual, family and environmental factors can increase a young person’s vulnerability to harm in terms of their mental and physical health and well being. Sometimes the harm caused can be significant. The challenge for services is to identify the most promising means of engaging with young people in order to divert them from behaviours that place them at risk for harm.
Think about the adolescents that you have on your caseload and have worked with in the past. Recall ways in which their behaviour was described and explained. List the kinds of stereotypes that you have heard, and maybe used.
Impact of Childhood Maltreatment on Adolescence and Risk Taking Behaviour
Patterns of child abuse and maltreatment can be divided into two main categories – abuse that has been continuous since early childhood, and abuse that begins during adolescence (Cawson et al, 2000, cited in Rees et al, 2010). Similarly, Moffatt has described how delinquent behaviour and criminality in adolescence and later life can be characterised in terms of early and late onset offending behaviour with regard to lifeourse criminality.
The legacy of early experiences of care and nurture can influence a young person’s ability to cope with outside influences (Brandon and Thorburn, 2008; Brown and Ward, 2013). Maltreatment in the early years can certainly affect brain development.Remaining in a family environment in which maltreatment has featured is also likely to increase a young person’s opportunities for risk-taking.
The Adverse Childhood Experiences (ACE) Study conducted in the US was a large-scale investigation into associations between childhood maltreatment and health and well-being in later life. More than 17,000 adults provided information about their childhood experience of abuse, neglect and family dysfunction. The study found that exposure to various forms of stress during childhood predicted later adverse forms of risk-taking. ‘In particular, such early stressors as physical and emotional abuse, emotional neglect, parental substance use, and exposure to violence in the household were linked to later adverse adolescent outcomes including drug use, addiction and suicide.’ (Romer, 2010) For females, experience of sexual abuse was strongly related to exposure to other sources of stress and linked to earlier age of first intercourse and unintended pregnancy. In general, the more adverse experiences an adult had had in childhood ‘the greater the emergence of risky behaviour in adolescence and later life’.
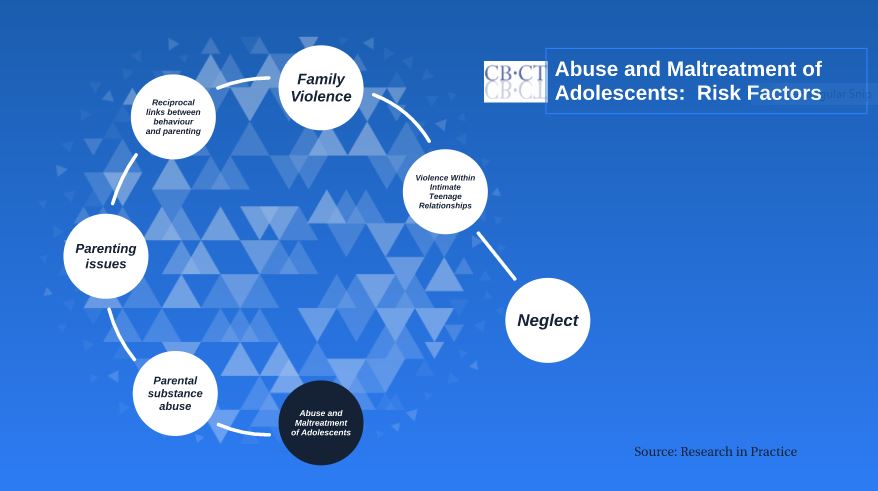
Abuse and Maltreatment of Adolescents
Summary
Throughout this module we have found common risk factors for mental health, challenging behaviour, substance misuse and vulnerability to exploitation and abuse, echoing the themes of Modules 1 and 2. As with the previous modules, the activities and resources on this page and subpage are intended to support the development of your knowledge base and build confidence in managing the challenging issues that lead to an increased risk of harm. The issues that arise for vulnerable adolescents are largely rooted in adverse Childhood Experiences and through these three modules we have identified the impact of individual characteristics of the child, their family and environment upon the child's development. We can also see how adults with similar early and childhood experiences may be vulnerable to a variety of problems that may undermine their ability and efforts to provide good parenting to their children.
The next two modules will focus on sexual abuse: Module 4 is concerned with adult perpetrators of abuse, patterns of abuse and its impact upon children and young people and our final module 5 addresses children and young people with sexually harmful behaviours.